
For most healthcare organizations, medical billing still lives in the back office. It’s treated as an administrative function. Something to manage and process, not something to learn from.
That gap creates a deeper problem. Clinical, operational, and administrative teams make decisions that directly impact revenue, but they lack visibility into financial outcomes. Poor visibility leads to weaker coordination and revenue management that reacts instead of strategizing.
As a result, financial performance falls out of line with day-to-day decisions.
The consequences show up in familiar ways. For example, in a 2024 Medical Group Management Association (MGMA) survey, 60% of medical group leaders reported rising claim denial rates—asign that payer requirements are outpacing current approaches. But denial rates only reflect part of the issue.
That’s driving a shift. More practices are moving toward a strategic revenue operations model. One that treats revenue as an organizational priority rather than a billing department problem. The shift brings clearer visibility to leadership, tighter alignment across departments, and a more consistent, data-informed approach to performance.
This guide covers how organizations can make that shift by building stronger healthcare revenue governance, improving cross-team coordination, and using revenue data to actually drive decisions.
Medical Billing Is Operationally Efficient But Strategically Invisible
Healthcare organizations are making progress in billing operations: faster claims, fewer errors, and more efficient workflows, thanks to advancements in medical billing software. But operational efficiency hasn’t translated into stronger financial performance.
The issue isn’t execution. It’s how organizations structure, govern, and use revenue.
Revenue Cycle Management Is Treated as a Back-Office Function, Not a Strategic Asset
Billing teams generally report to operations or administrative departments rather than executive leadership. As a result, revenue cycle management remains a support function, not a strategic priority.
Treating revenue as a back-office function amidst rising claim denial rates is financially risky. According to the American Hospital Association (AHA), administrative costs now account for 40% of the total cost of delivering care to patients in hospitals. This problem is prevalent across the board; independent medical practices and larger medical groups are also pouring resources into appealing and overturning inappropriate denials. The Journal of the American Health Information Management Association (AHIMA) reports that medical practices spend up to $25 on every first denial attempt.
Compounding this, operational costs are rising across the board. A 2024 MGMA stat poll shows that 92% of medical groups reported higher costs compared to 2023. Practices are spending more on physician salaries and staff wages, as well as on more expensive medical supplies and rising service and maintenance agreements.
Payer dynamics, regulatory complexity, and organization-wide decisions shape revenue performance long before a claim is submitted. But revenue isn’t governed at the level where those decisions happen. So no one is accountable for connecting them, and the strain of payer complexity and rising costs keeps pushing margins down and financial stress up.
That gap pushes organizations into recovery mode. Rather than improving performance at the source, they focus on denial management and appeals. According to a separate MGMA study, denials and appeals already represent the largest source of revenue leakage for nearly half of all medical practices.
Until revenue earns a seat at the executive table, organizations will keep chasing efficiency gains that don’t address the underlying structural problem.
Revenue Operations Impact Is Hidden Across Organizational Silos
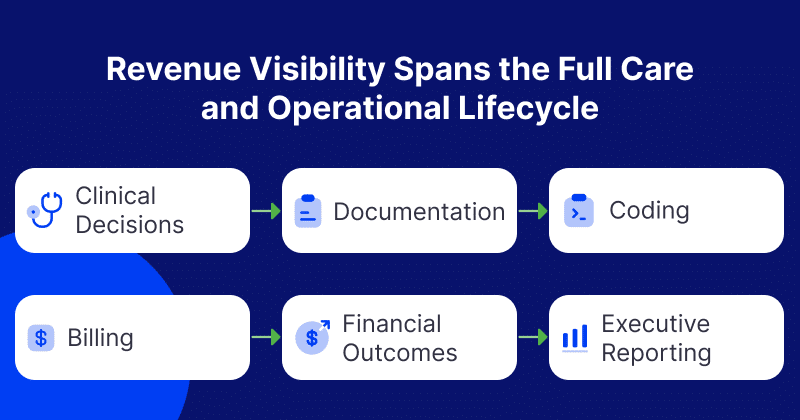
When revenue problems occur, they rarely start in billing. They start upstream in clinical, operational, and administrative decisions made by teams with no visibility into how their work affects financial outcomes.
Most healthcare organizations are structured to reinforce this. Clinical, operational, and revenue cycle teams report to different leaders, follow different goals, and track different metrics. No single team holds a complete picture of how revenue is generated or where it leaks.
The consequences are concrete. Scheduling teams typically focus on patient volume and access, not payer requirements like eligibility verification or prior authorization risk, yet denials often trace back to front-end issues. That means many revenue challenges are already in motion before a claim is submitted.
The problem isn’t individual team performance. It’s that no shared structure connects their decisions to financial outcomes. Each team optimizes for its own targets while revenue depends on how all those decisions interact.
The cost of this disconnection is high. According to the Healthcare Financial Management Association (HFMA), the administrative cost of reworking denials has reached nearly $20 billion annually, much of it avoidable. Those losses persist not because teams lack capability, but because the organization lacks alignment.
Siloed reporting keeps leadership in the dark. When financial, clinical, and operational data stay separate, it’s difficult to identify what’s driving performance or where revenue is eroding.
Fixing this requires shared reporting, aligned incentives, and clear ownership across every function that touches revenue.
Medical Billing Metrics Track Activity, Not Strategic Performance
Healthcare organizations generate enormous volumes of revenue data. Most of it tracks activity, not performance. Metrics like claims volume, denial rates, and collection timelines tell leadership what happened; they don’t explain why it happened or what to do next.
That gap is becoming harder to ignore. An analysis published by HFMA’s Greater Heartland Chapter revealed that 40% of health systems operated at a loss as of 2025, leaving little room for errors in decision-making.
At the same time, the Health Care Payment Learning & Action Network (HCPLAN) says 45.2% of U.S. healthcare payments now flow through alternative payment models. Of those, 28.5% carry downside risk. That environment demands a deeper understanding of what drives performance. Not just what performance looks like after the fact.
Yet most organizations still rely on backward-looking metrics that create a misleading sense of control. A low denial rate might suggest efficiency, but it says nothing about whether payer contracts are actually profitable. Faster collections may show process improvements while margin pressure and revenue leakage remain unaddressed.
Part of the problem is structural. Revenue metrics typically live inside billing or finance functions and don’t connect to clinical or operational decision-making. Leadership reviews financial performance through separate reports rather than a unified view. So revenue data stays isolated from the decisions that shape it.
The issue isn’t a shortage of data. It’s the absence of a framework that connects data to strategy. Metrics like service line profitability, payer contribution, and cost to collect rarely inform leadership decisions in any meaningful way.
Closing that gap requires integrating financial, clinical, and operational data into shared reporting that moves revenue beyond activity tracking and into strategic decision-making.
Revenue Cycle Management Is Reactive Instead of Predictive
Organizations still review performance after outcomes are set, rather than forecasting and adjusting in real time. Leadership relies on historical reports, limiting the ability to anticipate risks, identify trends, or adjust strategy.
This reactive model means leadership typically identifies revenue challenges, such as declining reimbursements, shifting payer dynamics, and underperforming service lines, after they impact financial performance.
The stakes of this approach are increasing. According to the 2023 HCPLAN report, 28.5% of U.S. healthcare payments carry downside financial risk, exposing organizations directly to performance variability rather than shielding them under fee-for-service models.
Without predictive visibility, organizations can’t model future revenue scenarios or assess how changes in volume, payer mix, or service mix will affect financial performance. That limits confidence in planning and makes it harder to:
- Invest in growth
- Allocate resources well
- Respond to market shifts
As a result, revenue cycle management remains focused on correcting past issues rather than proactively shaping future outcomes.
From Billing to Revenue Operations: A Structural Shift in Healthcare Finance
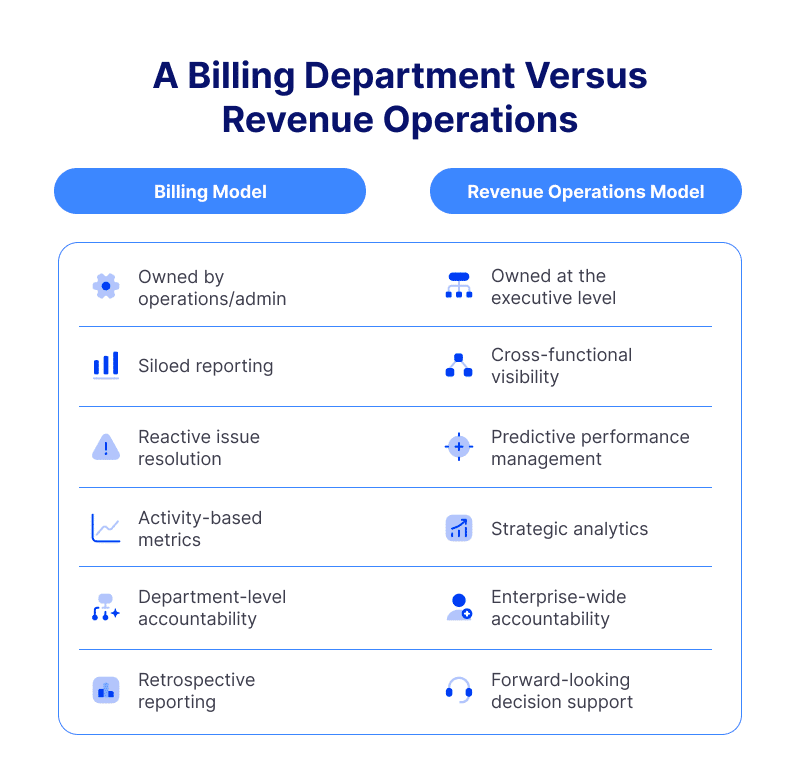
Better billing won’t fix a structural problem. Organizations need to rethink how they govern, own, and use revenue across the entire organization.
That’s what revenue operations does. The comparison below shows how it differs from traditional billing and what becomes possible when revenue management is aligned, accountable, and forward-looking.
The sections that follow break down how this model works in practice.
Revenue Operations Reframes Financial Performance as Strategy
In revenue operations, organizations treat revenue data as an input for decision-making rather than an outcome to be explained after the quarter closes.
This shift has practical implications. Leadership can use revenue insights to evaluate:
- Which service lines to grow
- Where to direct capital
- How to allocate resources
All based on actual financial impact rather than operational assumptions.
The industry is already moving in this direction. A 2024 HFMA survey found that 71.7% of healthcare executives identified revenue cycle technology as a top investment priority, and 77.6% plan to invest in automation. This shows a broader push toward more strategic, technology-enabled revenue cycle management.
But investment alone doesn’t close the gap. Many health systems still can’t analyze financial performance at the service-line or payer level, which means they can’t fully identify what’s actually driving profitability or where opportunity exists.
That’s the core problem revenue operations solves. When organizations build this visibility, revenue becomes a leading indicator of opportunities and risk. This keeps strategic decisions grounded in financial reality.
Executive Governance Elevates Revenue to a Strategic Function
Revenue operations redefines how revenue data is used. Governance determines who owns it and who’s accountable for it across the organization.
In a mature model, ownership sits at the executive level. The CFO or COO holds responsibility for revenue performance. A dedicated revenue operations leader reports directly to executive leadership. Shared dashboards connect clinical, operational, and financial data, and regular strategy reviews replace siloed billing meetings.
This shift is ongoing. In HFMA’s 2025 report, 88% of CFO respondents said they expect to spend more time on strategy over the next three years, while 63% expect to increase their focus on revenue cycle transformation.
Yet visibility remains a real barrier. Some organizations still lack integrated dashboards that bring financial, clinical, and operational data together. This leaves executives dependent on inadequate reporting that doesn’t support confident decision-making.
Organizations that close this gap see measurable results. Those with stronger analytics and governance collect faster and perform more consistently. These results confirm that executive-level accountability improves both how revenue is managed and what is ultimately delivered.
When governance is in place, revenue is no longer just one department’s job. Leadership owns it, teams track it with shared metrics, and everyone works together to improve it.
Cross-Functional Visibility Aligns Clinical, Operational, and Financial Decisions
Most organizations track activity. Revenue operations teams track impact.
That distinction matters because activity metrics—volumes, timelines, and transaction counts— tell teams what happened.
Strategic analytics tell teams:
- Which service lines are profitable
- Which payers contribute positively
- Where financial sustainability is at risk
Shared reporting connects this data flow and gives all teams a common understanding of performance.
Right now, most organizations aren’t using this data. According to the World Economic Forum, up to 97% of hospital data goes unused, leaving significant analytical value untapped. The cost of that gap is real.
When organizations connect financial outcomes to the clinical and operational drivers behind them, leadership gains a clearer understanding of what’s actually moving performance and where value is being created or lost.
Revenue data stops being a reporting output and starts functioning as a decision-making asset, supporting smarter choices around growth, resource allocation, and long-term financial strategy.
Predictive Infrastructure Enables Proactive Revenue Cycle Management
A revenue operations model introduces predictive capabilities. It enables leadership to get ahead of revenue problems rather than responding to them.
With the right infrastructure, organizations can:
- Forecast performance
- Model how changes in payer mix or service offerings will affect revenue
- Surface risks before they show up in financial results
The value of this approach is already evident. Organizations using advanced analytics and population health capabilities have seen up to 24% lower hospital admissions and more than 30% lower readmission rates, according to the Milbank Memorial Fund report. This demonstrates what proactive, data-driven decision-making can produce at scale.
That same predictive visibility applies directly to financial planning. When leadership can plan future scenarios rather than just review past ones:
- Budgeting becomes more grounded
- Resource allocation improves
- Strategic decisions carry more confidence
As a result, revenue cycle management shifts from reacting to past performance to actively shaping future outcomes.
What Revenue Operations Unlocks: Financial Performance as Competitive Advantage
A revenue operations model doesn’t just change how organizations analyze revenue. It changes who owns it, how teams align around it, and how leadership uses it to make decisions.
Accountability shifts first. Revenue moves to the executive level, under the CFO or COO, so leadership manages it as an ongoing priority rather than reviewing results after the fact.
Reporting follows. Shared dashboards replace fragmented, department-level reports, connecting clinical, operational, and financial data so leadership can link decisions to outcomes and respond earlier.
Teams start working from the same picture. Clinical, front-end, and billing functions align around shared performance data instead of operating in silos. A 2024 HFMA report shows 40.9% of organizations already focus on revenue integrity, and 40.2% are investing in EHR optimization; both signal a broader shift from traditional billing toward revenue operations.
Organizations that rely on fragmented reporting and operational metrics will struggle to compete in a more performance-driven environment.
Platforms like CollaborateMD help organizations make this shift, connecting reporting, scaling billing operations, and building the visibility needed to manage revenue as a strategic function. Organizations that invest in this infrastructure now can better manage complexity, strengthen financial resilience, and perform consistently over the long term.