
The traditional revenue cycle management (RCM) model is breaking under the weight of its own complexity. Initial claim denial rates have climbed to nearly 12%, resulting in an estimated $262 billion in denials annually across the U.S. According to a CAQH report, the entire U.S. medical industry spends an estimated $83 billion annually on staff time to conduct routine administrative transactions, with providers shouldering 97% of those costs.
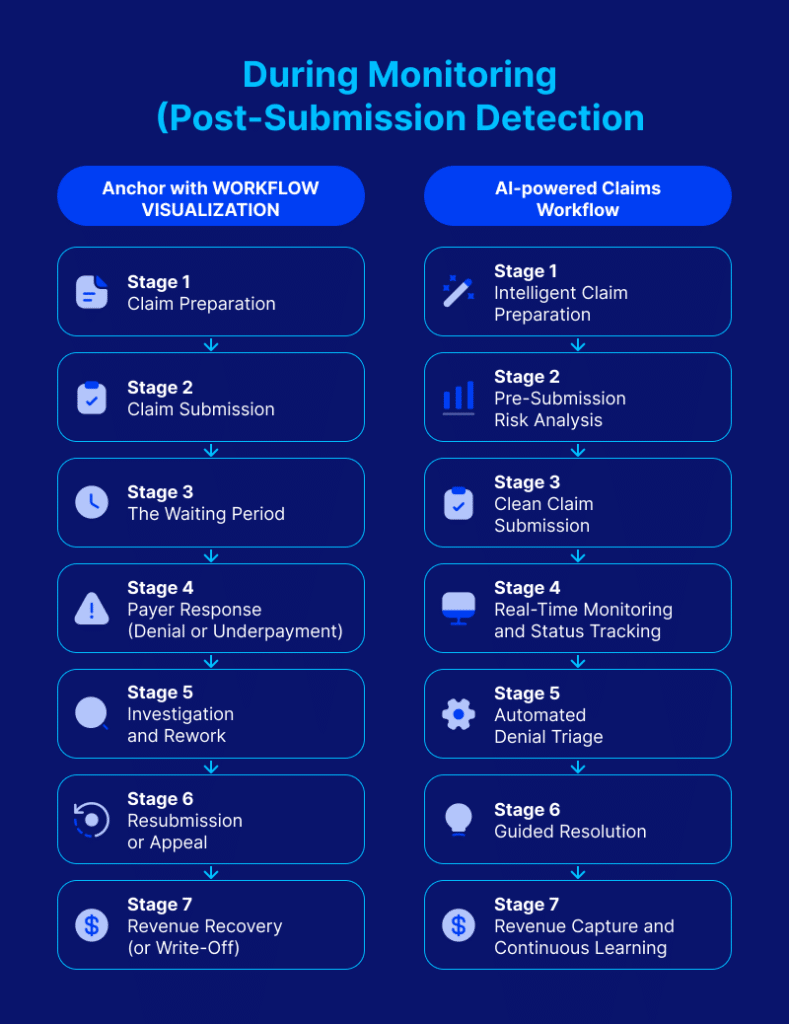
The problem is one of timing. Traditional revenue cycle workflows are built on detection and correction: submit a claim, wait for a response, discover a problem, and fix it after the fact. Every stage of that cycle introduces a delay, and delay is where revenue leaks.
AI-powered automation changes the timing of intervention by continuously monitoring claims, predicting denial risk, and surfacing intervention opportunities before problems become write-offs. This represents an opportunity for operational transformation, not just an incremental improvement, and it has measurable consequences for cash flow, staff efficiency, denial rates, and financial predictability. It’s a shift that CollaborateMD by EverHealth is actively leading, and understanding this opportunity starts with a closer look at where traditional revenue cycle management breaks down.
How Traditional Revenue Cycle Management Is Reactive
Revenue cycle management in clinical practices has become extraordinarily complex. It spans patient registration, insurance verification, charge capture, coding, claim submission, remittance processing, denial management, and patient collections. As the journal Cureus points out, this is a process prone to errors at every handoff point.
Although reimbursement rates for service codes are preset and services are documented, the system introduces friction through denials, prior authorization requirements, coding ambiguity, and payer-specific rules that vary across contracts. As a result, billing teams spend most of their time reacting to problems that have already occurred instead of preventing them.
Three structural forces have made the reactive model unsustainable, and all three are compounding simultaneously.
First, payers have invested in denial infrastructure, which is causing denials to increase. Denied amounts rose 12% for inpatient and 14% for outpatient claims in 2025. External payer audits showed a 30% year-over-year increase in total at-risk amounts. When denials occurred, the average outpatient denied amount was $5,390.
Second, regulatory agencies have expanded documentation requirements and audit authority. There’s constantly more paperwork, more compliance checkpoints, and more stress on administrative and billing staff. All of this is happening without corresponding increases in staffing or tooling.
Third, staffing shortages have reached critical levels. According to the journal, Risk Management and Healthcare Policy, staffing shortages burdened hospitals with $24 billion in 2021 alone. Without enough staff, hospitals are forced to rely on agency staff and pay existing workers overtime to fill critically needed positions, dramatically increasing labor costs. These staff shortages impact independent practices as well. A 2024 survey conducted by the Medical Group Management Association (MGMA) found that 53% of medical group leaders say finding candidates is their top staffing challenge. Practices are struggling to fill admin roles, as well as revenue cycle management roles, coders, medical assistants, and nurse practitioners.
Let’s further explore how these problems compound at different stages of revenue management.
At Submission (Pre-Claim Issues)
Patient eligibility verification gaps are one of the leading causes of preventable denials. Yet, in the traditional model, verification happens manually and inconsistently, which increases the risk of errors.
Prior authorization has also become one of the most resource-intensive bottlenecks in the pre-claim process. Data from the American Medical Association (AMA) shows that practices complete an average of 39 prior authorization requests per physician, per week, and physicians and staff spend 13 hours weekly on those requests alone.
A peer-reviewed Health Affairs Scholar study also found that provider organizations spend the time equivalent of 100,000 full-time registered nurses per year on prior authorization (PA) activities. Billing and coding specialists average 11 hours per week on PAs alone. Finally, 93% of physicians report that prior authorization causes care delays, and 82% say it can lead to treatment abandonment, according to an AMA survey.
Coding errors before submission also compound the problem. In a manual environment, coding accuracy depends entirely on coder bandwidth and familiarity with payer-specific rules, both of which are under pressure from volume and staffing constraints.
Once a claim is submitted, traditional workflows rely on manual tracking and delayed feedback loops. Unfortunately, teams often don’t know a claim has stalled until they actively go looking for it or a denial arrives. McKinsey’s analysis of the revenue cycle describes how disconnected systems create blind spots. When EHRs, medical billing platforms, and clearinghouses don’t share data in real time, claim status monitoring becomes a manual, labor-intensive exercise that can’t scale with volume.
High claim volumes also make manual monitoring functionally impossible at scale. The sheer number of claims moving through the system means that by the time a team identifies an issue, the optimal intervention window has often closed. For practices relying on disconnected systems, no single view of claim status exists, and teams piece together information from multiple platforms to understand where a claim stands.
Consider a mid-sized practice managing claims across four separate platforms: one for EHR documentation, another for billing, a third for scheduling, and a fourth for clearinghouse connectivity. When a claim stalls, there’s no single dashboard that tells the team why. A billing specialist has to log into each system individually, cross-reference timestamps and status codes, and manually reconstruct the claim’s journey. Multiply that across hundreds of claims per week, and the monitoring process alone becomes a full-time job that still can’t catch every issue in time.
At Intervention (When Problems Surface)
In the traditional model, problems surface primarily through denial notifications, which arrive days or weeks after submission. This is long past the point where a quick correction would have resolved the issue, and unfortunately, the consequences pile up. Forty-one percent of healthcare providers now report that more than one in 10 claims is denied, which is up from 30% just three years ago.
The American Hospital Association (AHA) also states that nearly 15% of all claims submitted to private payers are initially denied, including many that had prior authorization approval. Late-stage denial discovery forces teams into reactive correction mode—researching the denial reason, gathering documentation, and resubmitting or appealing. All of these are resource-intensive tasks that could have been prevented with earlier intervention. Claim denials can cost more than $100 to rework.
Through Resolution (Cleanup Costs)
The financial consequences of reactive resolution compound over time. According to the Healthcare Financial Management Association (HFMA), true accounts receivable days increased by 5.4% year-to-date in late 2024. This was driven by a 17% increase in request-for-information denial rates and a 7% increase in initial denial rates for inpatient commercial claims.
Up to 65% of denied claims are never reworked at all. Of the 54.3% denied claims that are ultimately overturned, the reversal comes only after multiple rounds of costly appeals. Moreover, staff burnout from constant firefighting erodes institutional knowledge and drives turnover, which further degrades the revenue cycle.
The cumulative result is revenue unpredictability. When you can’t predict which claims will be denied, how long resolution will take, or how much revenue will be written off, financial planning becomes guesswork.
How AI Automation Focuses on Prediction and Prevention
The shift from reactive to proactive revenue operations isn’t meant to replace billing teams. Instead, the shift aims to change when and how problems are identified so that teams can act before revenue is at risk.
It’s no surprise that the fastest-growing use case for predictive AI from 2023 to 2024 was for simplifying or automating billing procedures. According to the Office of the National Coordinator for Health Information Technology, usage grew from 36% in 2023 to 61% in 2024. AI-powered automation continuously monitors claims, predicts denial risks, and surfaces intervention opportunities before problems occur. Let’s explore each use case in more detail.
Flags Issues Early
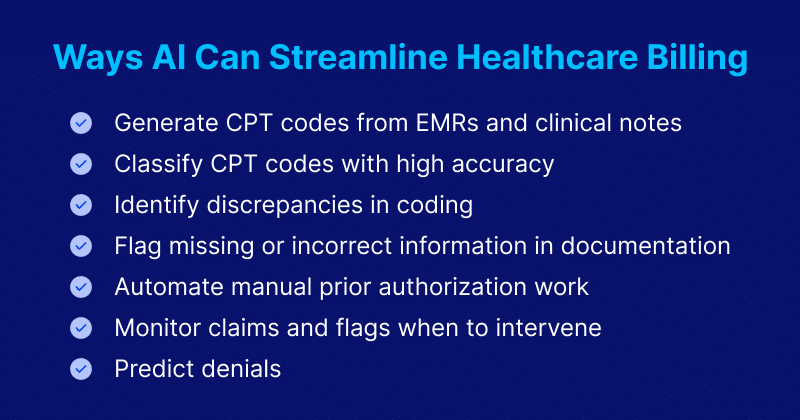
Intelligent claim rejection helps decode vague payer messages and reduces rework and claim delays by offering simple AI-generated explanations of payer rejections codes.AI-powered claim scrubbing identifies coding errors, missing modifiers, and documentation gaps in real time. This happens before the claim is submitted, not after a denial comes back. The data is clear on how effective this AI-powered process can be.
Furthermore, a Midwest health system that deployed a denial prediction AI model integrated with its EHR reduced denial rates by 18% and improved first-pass yield from 85% to 92%. This translated to $40 million in additional net revenue in a single year.
The system learns over time from recurring denial patterns and applies that learning to flag high-risk claims before submission. For instance, the system might learn that a specific payer consistently denies claims with a particular modifier combination, or that a certain procedure code triggers denials when submitted without supporting documentation that other payers don’t require. Over time, it builds a payer-specific risk profile that flags these claims before submission by surfacing the exact documentation gap or coding pattern that’s likely to cause a rejection. This kind of granular, learned intelligence is something manual review teams simply can’t replicate across thousands of claims with dozens of payer rule sets.
AI also monitors for prior authorization requirements and alerts staff when an authorization is missing or about to expire. This addresses one of the most time-intensive pre-claim bottlenecks for revenue management teams.
Increases Staff Efficiency
AI automates the highest-volume, most repetitive tasks in the revenue cycle: eligibility verification, claim status inquiries, payment posting, and remittance reconciliation. These are tasks that previously required manual search across multiple systems. AI-powered data import claim entry can be streamlined with AI-powered Universal Import. By importing patient encounter data from any EHR in minutes-not hours of manual claim entry- staff save valuable time and data is more accurate so there are less errors and rework- turning raw files into billing-ready claims.
In a traditional workflow, a billing specialist might manually verify eligibility for each patient encounter, check claim status by logging into payer portals individually, and reconcile payments against the expected amount by hand. AI handles these tasks at scale, in seconds, continuously.
AI-assisted coding also validates codes against payer-specific rules and clinical documentation in real-time, which reduces the back-and-forth between coders and clinicians. Reducing bottlenecks in this way is likely why organizations implementing explainable AI for coding see a 25% to 50% reduction in code-related denials.
Automated alerts surface the claims that need human attention. Rather than requiring staff to review all claims, the system triages by risk and routes exceptions to the right person with the relevant context already attached. This shifts staff from doing the work to overseeing the work. The role evolves from data entry and manual lookup to exception management, compliance review, and strategic decision-making.
Optimizes Revenue Cycle Performance
Beyond individual claim accuracy, AI-powered systems optimize the revenue cycle as a whole by continuously monitoring the pipeline and identifying systemic issues. For example, a payer that’s consistently denying a specific code, a provider whose documentation patterns lead to higher denial rates, or a claim type with an unusually long resolution time are potential issues AI can keep track of.
Predictive models also assess expected reimbursement amounts against actual payments, flagging underpayments and contract variances that would otherwise go unnoticed until month-end reconciliation (or never). Real-time revenue pipeline visibility replaces backward-looking monthly reports with continuous monitoring, giving practice leaders the ability to see where revenue stands at any point and intervene before shortfalls materialize. This is what shifts revenue management from a reporting function to an operating function.
The Potential Impact of Intelligent Revenue Management in Healthcare
Understanding how AI-powered automation works is only half the equation. What matters to practice leaders is what it means for the business. The impact extends across four dimensions: financial performance, operational scalability, strategic decision-making, and the patient experience.
Financial Impact
The financial case for AI in revenue cycle management is grounded in measurable, near-term metrics. These include, but aren’t limited to, days in A/R, denial rates, first-pass yield, and net collection rate.
True accounts receivable days may have increased in 2024, but practices that can reverse that trend through earlier intervention can gain a direct cash flow advantage. Every denial that’s prevented is a claim that doesn’t require rework, appeal, or write-off, and at the high cost of reworking claims, prevention is significantly cheaper than correction.
AI also shortens the time in accounts receivable by identifying and resolving issues earlier in the lifecycle, which directly accelerates cash conversion. For instance, the U.S. healthcare system avoided an estimated $258 billion in administrative costs in 2024 through electronic and automated transactions. That’s a 17% increase in cost avoidance over 2023. However, the gap between what’s being saved and what remains on the table represents a significant financial opportunity.
Operational Impact
The operational impact extends beyond efficiency gains for individual staff. It also changes the scalability of the revenue cycle function itself.
With AI handling routine verification, status checks, and claim triage, the same team can manage a larger volume of claims without a proportional increase in headcount. This is critical given staffing gaps.
Automation provides a structure and answer to a workforce problem that hiring alone cannot solve. According to MGMA, medical practice leaders reported an average year-to-date operating expense increase of 11.1% in 2025, with 90% of medical groups reporting rising costs. However, AI-powered automation is one of the few levers that can improve output while reducing marginal cost, which is the opposite of the traditional “hire more people” approach.
There’s also the downstream operational benefit of stress and burnout relief. Fifty-four percent of physicians believe AI can help with stress and burnout, and 48% believe AI can address cognitive overload.
Strategic Impact
Intelligent revenue operations give practice leaders something the reactive model can’t: predictability. For example, CFOs can forecast with confidence when the revenue pipeline is visible in real time rather than reconstructed from month-end reports. Better cash flow planning, via 90-day revenue visibility instead of a 7-day window, enables more accurate budgeting, smarter resource allocation, and the ability to make strategic investments instead of hoarding cash against uncertainty.
AI also enables data-driven decision-making across the practice. Service line profitability can be analyzed based on actual collection data rather than charge data. Teams can negotiate payer contracts using leverage based on denial pattern intelligence. And leaders can optimize staff based on predictable workload instead of reactive crisis management.
Patient Experience Impact
More than half of consumers in the U.S. report experiencing at least one problem when paying for healthcare. These problems can include billing confusion, unexpected charges, delayed statements, and unresolved disputes, which all erode trust in the system that’s supposed to care for them.
When the revenue cycle operates proactively, patients benefit from accurate estimates before service, fewer surprise bills, faster claim resolution, and clearer communication about their financial responsibilities. AI-driven revenue cycle workflows eliminate the payment issues discussed above, and faster resolution also means fewer patient calls to the billing office asking about claim status. This further reduces administrative workload and improves the patient’s perception of the practice.
Implementing AI in Medical Billing: Ethical and Practical Considerations
The operational case for AI in revenue cycle management is strong, but adoption introduces responsibilities that can’t be treated as afterthoughts. These include transparency, data privacy, human oversight, and bias mitigation. Knowing how to approach these factors, as well as practical considerations, can help your practice avoid costly missteps and implement sustainable AI adoption.
Integration and ease of use are the primary practical considerations when implementing AI. A system that requires a full rip-and-replace of existing infrastructure will stall at procurement. McKinsey’s report cited earlier identifies sequencing and integration as key success factors for revenue cycle automation. Specifically, organizations that pilot AI in targeted areas, like claim scrubbing or eligibility verification, before scaling, see faster adoption and better results.
However, there are valid reasons for hesitation, such as skill gaps, concerns about implementation downtime, and uncertainty about ROI. The answer is choosing a partner with fast implementation, easy navigation for front-of-house and billing staff, and a track record of supporting practices through the transition, not abandoning the project entirely.
AI transparency and explainability are also important considerations. The Centers for Medicare and Medicaid Services (CMS) Program Integrity Manual, the False Claims Act’s 60-day overpayment rule, and the 21st Century Cures Act all demand that healthcare organizations demonstrate clinical evidence, guideline logic, and version history behind coding. When the system can explain why it chose a code, auditors and payers can verify it.
Transparency also matters for staff trust and adoption. If billers and coders can’t understand why the system flagged a claim, they won’t trust its recommendations.
AI tools that process protected health information must also comply with HIPAA regulations. In January 2025, the Health and Human Services Department (HHS) published a proposed rule to revise the HIPAA Security Rule, establishing that the ePHI used in AI training data, prediction models, and algorithm data is protected by HIPAA. This means that AI tools must be designed to access only the minimum necessary PHI for their purpose, with audit trails and access controls.
Knowing this, it makes sense that half of healthcare leaders cite data privacy and security concerns as the biggest barrier to AI adoption. Choosing a provider with built-in compliance infrastructure addresses this concern directly.
It’s also important not to get carried away with the potential of AI. This technology plays a supportive role, meaning that it augments human judgment, but it can’t and shouldn’t replace it. This means that in any AI-powered automation integration, human oversight remains essential for complex claims, exception handling, and compliance review. AI frees staff to focus on exactly these high-judgement tasks by handling routine work at scale.
Bias in predictive models is another real concern. Health Affairs research found that although most U.S. hospitals use predictive models, fewer than half systematically evaluate those models for bias. However, training data or algorithm design flaws can lead to inequitable billing practices. Ensuring diverse and representative datasets combined with thorough validation processes can help mitigate bias risk.
Without transparent model training and bias mitigation protocols, AI risks undermining the very adoption it’s trying to drive, so it’s important to carefully evaluate these protocols before choosing an integration partner.
Moving into a New Era of Revenue Cycle Management with AI Automation
The traditional revenue cycle was designed for a healthcare system that no longer exists. Claim volumes were lower, payer rules were simpler, and manual processes could keep up with demand. That era is over. Denial rates are climbing, staffing gaps are widening, operating costs are rising at double-digit rates, and the reactive model of submit-wait-discover-fix can’t sustain financial performance under these conditions.
AI-powered automation addresses this not by asking billing teams to work harder when they’re already past their limits, but by changing when problems are identified and resolved. When eligibility gets verified before the patient leaves the office, or when coding errors are caught before submission, or even when denial risk is predicted and mitigated before the claim reaches the payer, the entire downstream cascade of rework, write-offs, and revenue unpredictability diminishes.
The result is measurable in lower denial rates, shorter A/R cycles, higher first-pass yield, and a revenue operation that can scale without scaling headcount. CollaborateMD is building toward this future by partnering with practices to move from reactive cleanup to intelligent, proactive revenue operations. Talk to our team to see how CollaborateMD can transform your revenue cycle.